DIVERTICULITIS
(text automatically translated from Greek)
What is diverticulitis?
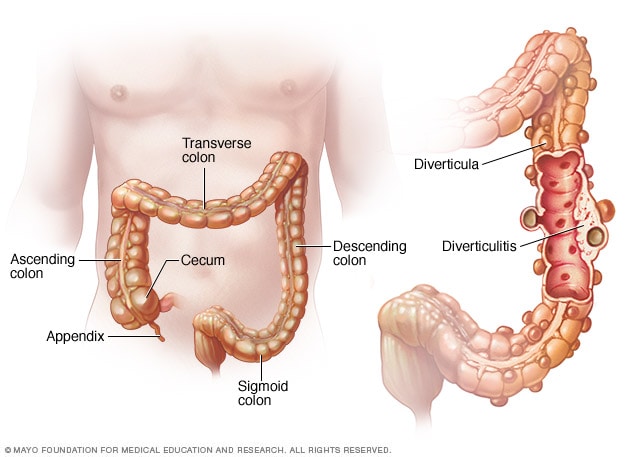
Diverticula are small blisters that protrude through the muscular wall of the colon. Occasionally, diversions also occur in the small intestine, stomach, and esophagus. Many people have diversions without causing them any problems. Diverticulitis occurs when one or more diverticula become infected or broken. The incidence of diversions increases with age. In the US, more than 50% of people over the age of 70 have diverticula, but only a small percentage of people actually develop diverticulitis. The presence of diversions is more common in women than men and occurs mainly in Western cultures.
What causes diverticulitis?
The exact reason for the formation of diversions is not known, but it is believed to be a result of the increasing amounts of flour and sugar in the western diet. Diverticula are rare in less developed countries where the diet is higher in fiber. However, overconsumption of legumes also leads to increased gas volumes in the large intestine. It is believed that food and the accumulation of gas in the large intestine can cause increased pressure on weak (weak) points of the intestinal wall, causing the gradual development of diversions. Chronic constipation is probably a high risk factor for developing this condition. Stress, tension and mental stress can all cause increased bowel contractions, which can also contribute to the formation of diversions. Infection occurs when the diverticulum stretches and ruptures, causing small pericardial abscesses to form. This leads to inflammation, which in turn can cause further complications. Inflammation can remain in the areas where it develops or through a large rupture can spread throughout the abdomen.
What are the symptoms of diverticulitis?
While many people with diverticulitis do not develop diverticulitis as the diverticula grow or become transiently inflamed, the large intestine becomes narrower and narrower and this can cause problems (chronic constipation, incomplete ileus). In addition, in some people with diversion, the colon muscle becomes thicker and thicker, making it narrower. This combination of diverticula and abnormal muscle thickening is referred to as diverticular disease.
Symptoms of diverticulitis include pain along the large intestine and a change in bowel habits , with the passing of pellet-like stools after significant difficulty in emptying. Another common symptom is frequent bloating and flatulence. Occasionally, small amounts of blood may pass through the bowel movements. These symptoms are very similar to those seen in irritable bowel syndrome (IBS).
Acute diverticulitis occurs when one or more diverticula become infected and inflamed. The pain is usually felt on the lower left side of the abdomen, but sometimes appears on the right side (when there is a very long sigmoid). Other symptoms include fever, high white blood cell counts (indicating a microbial infection), loss of appetite, and nausea . Peritonitis _is a serious complication of diverticulitis that occurs when one of the diverticula breaks and germs spread to the abdominal cavity. Neglected cases develop communication of the colon with the bladder (fistula), resulting in frequent urinary tract infections and the finding of air in the urine (foamy urine).
ROBOTIC TREATMENT DISEASE
In the event of multiple recurrent episodes of diverticulitis, your doctor will recommend a colectomy , which is a surgical removal of part of the colon. Depending on the part of the intestine that is removed, the colectomy is called right, left, sigmoidectomy, low anterior colectomy or abdominal perineum (usually sigmoidectomy for diverticulitis). The removal of part of the intestine is now performed laparoscopically, ie through 4-5 small holes in the abdominal wall with a diameter of 0.5-1 cm while the classic (open) removal remains useful in cases where the laparoscopic technique is not possible. Robotic Bowel Removal is an evolution of laparoscopy, performed using a robotic system and offers a better imaging of the surgical field (three-dimensional, high-resolution stereoscopic) and greater ease of intraoperative manipulations (articulated tools with seven degrees of freedom). New technologies coming as robotic additives, such as the use of ICG (firefly fluorescence) fluidscence can assist these operations by providing more information about the anatomy and location of the lymph nodes and the perfusion of the intestinal parts to be reunited (assessment of vascula ). Studies show lower rates of conversion to open surgery using the robotic technique,
During the laparoscopic or robotic colectomy, the surgeon SK Chiridis, after gaining access to the abdomen and injecting gas (carbon dioxide) to create the necessary workplace (pneumoperitoneum), will first check the entire abdomen. It will then cut any adhesions (reactive tissue in the abdomen) around the affected area of the intestine. In bowel surgeries and especially in cases where malignancy is suspected, the most current data dictate control of the intestinal vessels early in the operation (medial-to-lateral approach) without manipulations in the area of the suspicious mass (no touch technique). These vessels are prepared and cut low near their protrusion to include all the lymph nodes in the area (lymph node dissection - total resection of the intercostal space). In the right and left colectomy, after ligation of the vessels of the intercostal space, the intestine is carefully detached from the lateral abdominal wall. In the case of the rectum, it is important to perform the total mesorectal excision (TME), ie the perioral fat and all the perioral lymph nodes. When the affected part is completely released, it is removed from a small incision in the lower abdomen. After the closure of the abdominal wall, the wounds are sutured intradermally and the skin is contracted in its original position. that is, the perioral fat and all the perioral lymph nodes. When the affected part is completely released, it is removed from a small incision in the lower abdomen. After the closure of the abdominal wall, the wounds are sutured intradermally and the skin is contracted in its original position. that is, the perioral fat and all the perioral lymph nodes. When the affected part is completely released, it is removed from a small incision in the lower abdomen. After the closure of the abdominal wall, the wounds are sutured intradermally and the skin is contracted in its original position.
Dr. Chiridis is the first surgeon of his generation to be trained in Robotic Surgery in Greece . From January 2007 to August 2017, Dr..S.Khiridis worked at the Clinic of General, Laparoscopic and Robotic Surgery of the Athens Medical Center (Director: KM Konstantinidis), and actively participated in the first Greek Robo Program. Surgery with a total experience of more than 3500 surgeries. At the same time , he specialized in Hernia Robotics, Upper and Lower Digestive and Robotic Manual of Obesity - Metabolic Diseases.
During his specialty at the General Hospital of Athens, the doctor gained extensive experience in the full range of open surgery of the small and large intestine , knowledge necessary before proceeding with the least traumatic techniques.
He then completed with a scholarship the Postgraduate Program in Robotic Surgery of the Medical School of the National & Kapodistrian University of Athens for the title "Master of Science" (MSc) and received the title of Doctor of the University of Athens (PhD) for his research in Metabolism.
His first formal training in Robotic Surgery was in early 2007 at the University Hospital of Grosseto, Italy , a small town outside Siena, where the internationally renowned robotic liver-pancreas surgeon Pierro Giullanotti was then working. Close to this great surgeon and his team (Dr. Chiridis's trainer in the laboratory was the now famous Indian surgeon, Jay Deep Palep), Dr. Chiridis was trained in the basic principles of robotic system setup, use of the control console, change of tools and performed cholecystectomy on an animal model. He also had the opportunity to attend pancreas surgeries by the famous Italian team currently based at the University of Illinois, USA.
This first training was followed by a large series of advanced trainings in Advanced Laparoscopy in international referral centers abroad (Strasbourg - advanced laparoscopic surgery course (included practice in laparoscopic surgery of Nissen vaulting and single - splicectomy course), Geneva advanced course on minimally invasive upper and lower GI surgery, Vienna - advanced course on ventral and inguinal hernia surgery, Amsterdam - MIS for benign and malignant pelvic disease, Frankfurt - masterclass on hiatal hernia and GERD - Seminar on specialization in septal surgery and hernia ).
In 2009, Dr. Chiridis traveled to Houston-Texas to train in one of the first international meetings of Robotic Surgical Oncology, held at the renowned MD Anderson Oncology Reference Center (PAROS meeting 2009).
In the same year he presented 6 pioneering works of Robotic Surgery at the 19th International Congress of IASGO in Beijing , China (19th World Congress of the International Association of Surgeons, Gastroenterologists, and Oncologists (IASGO), Beijing, China).
That same year in Chicago (ACS Clinical Congress) , he had the opportunity to test the new dual training console as well as the (experimental at the time) Single Site Robotic Platform at the invitation of the manufacturer.
In December 2009 he was elected General Secretary of the Hellenic Scientific Society of Robotic Surgery and remains in this position until today .
In October 2010, the Board of Directors of the International Community of Robotic Surgery MIRA appointed him to co-chair with the internationally renowned robotic surgeon Ivo Broeders, in the Scientific Program of the 2011 MIRA World Conference on Robotic Surgery.
In the same year he successfully completed the Course and Laboratory Session in Robotic Colorectal Surgery (Hands-on) of UC University San Diego . There he had the opportunity to be trained in Robotic Colon Surgery with an emphasis on the robotic technique of Total Robin TM (robotic TME) and practical training in the laboratory, in cadaver donors.
In January 2011, together with the Medical team, they were the first in the world to be trained in Robotic Cholecystectomy Without Incisions in France and applied it as soon as they returned, simultaneously with a center in Italy and one in Switzerland.
In September 2012, Savvas Chiridis won the silver medal among 75 participants from all over the world at the annual Robotic Surgical Simulation Olympics Olympiad as part of the SLS-MIRA-SRS 2012 International Conference in Boston, USA. . At the same meeting, the doctor received two awards for best video presentation that he had edited and sent himself, representing the team of the Athens Medical Center .
He then trained in Advanced Upper and Lower Digestive Robotic Surgery in Bucharest (Professor Irinel Popescu) and Robotic Thyroidectomy with Neurophysiological Monitoring in Cluj-Napoca (Professor Constantea).
In July 2012 he participated as an instructor in the first hands-on robotics course in Greece which took place in the laboratories of the pharmaceutical company ELPEN.
In January 2013 he attended the work of the clinic and the operations of the internationally renowned robotic surgeon and good friend Fabrizio Luca at the IEO / European Institute of Oncology in Milan, Italy. This clinic is considered a center of reference in Robotic Colon Surgery and its then director is also in America today. Dr. There, Chiridis optimized his knowledge of very low anterior colectomy and robotic TME in rectal cancer.
In October 2013 he successfully completed the skills course Laparoscopic and Robotic Colon Surgery in Washington DC, USA.
In November 2014 , Dr. surgery of the Athens Medical Center.
In 2015, in the context of the launch of the first robotic program in Cyprus, Dr. Cheiridis was trained in the new da Vinci Xi robotic system by the manufacturer, at the American Medical Center, Nicosia.
Together with the Robotic Surgery team of the Athens Medical Center, Dr. Chiridis contributed to the launch of the first Robotic Surgery Program in Thessaloniki (Inter-Balkan Medical, Professor Dr. Basdanis), in Cyprus (American Medical Center, Nicosia), and Sofia (Dovere Hospital).
He has numerous publications in Greek and foreign journals, has participated in the writing of many medical books and participates as a guest speaker at international conferences of Robotic Surgery in Europe (Stockholm, Seville, Prague, Geneva, Turin, Brussels, Brussels, Brussels). , Sofia, Bucharest, Amsterdam) of America (Quebec, Chicago, Boston, San Diego, San Francisco) and Asia (Beijing).
He is a member of the Hellenic Society of Surgery, the European Society of Laparoscopic Surgery (EAES), the International Society of Robotic Surgery (SRS), and the American College of Surgeons (FACS) .
Today he performs robotic surgeries from the whole spectrum of General Surgery (surgery of abdominal wall hernia, septal hernia and reflux, stomach, gallbladder, small & large intestine, anus and perianal diseases and morbid obesity in Cyprus and obesity in Greece). His patients are completely satisfied with both the choice of robotics and the choice of robotic surgeon Dr. Savvas K. Heiridis.